Political/World Issues
What is Abortion?
So many people have no idea. Amazingly many people who oppose it have little knowledge of what abortion actually is. I have come to believe that it is a major reason why we don't do anything about it. If you knew, you couldn't help but desire to do something. You would do something.
Abortion
has become a word that has lost it's definition, a political term bantered back and forth. We have become callous towards a word that
means so much more than “a legal and safe way to end pregnancy”,
as Planned Parenthood defines it. It's more than “a forced removal
of a fetus from the womb”, as Wikipedia describes.
This
became apparent to me when I decided to educate myself on the
procedures of abortion. I was disturbed. No, that's an
understatement. My soul weeps and I am left speechless and in
horror. Do you have any idea?
Prepare yourself -- once you know you will be moved into action. Doing nothing will no longer be an option.
(The following includes some graphic illustrations and photos along with detailed information on the procedures of abortion methods. This post would be inappropriate for young children under twelve).
SUCTION
CURETTAGE OR VACUUM ASPIRATION ABORTION:
The Stats:
Suction
curettage (or vacuum aspiration) abortion is the most commonly used
method of abortion around the world. This is because most abortions are performed in the first trimester.
The National Abortion
Federation (NAF) has reported that
"...virtually
all modern first-trimester surgical abortions are accomplished by
vacuum aspiration." 1
The Procedure:
 Firstly, a speculum is placed in the vagina, a tenaculum is clamped to the lip of the cervix, and a cannula is inserted into the uterus.
Firstly, a speculum is placed in the vagina, a tenaculum is clamped to the lip of the cervix, and a cannula is inserted into the uterus.
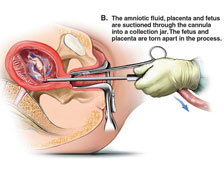
Secondly, the amniotic fluid, placenta and fetus are suctioned through the cannula into a collection jar. The fetus and the placenta are torn apart in the process.

Lastly, the uterine cavity is scraped with a curette to determine if any tissue remains.
Although the suction curettage method isn't commonly used after 12 weeks gestation.
12
week embryo:

To confirm and complete an abortion the embryos tissue must be examined after the abortion has been completed. Small embryo parts are apparent at even 9 weeks gestation "and become easier to identify thereafter."
If body parts are too large the the abortionist uses " a ring forceps to remove any material that is wedged in
the end of the cannula or lodged at the external
os."5
The Doctor's Description:
Warren
Hern (author of Abortion Practice) describes his post-abortion procedure this way:
As the
physician completes the procedure, he should inform the patient that
the procedure is being completed… Keeping the vaginal bimanual
examination hand sterile, the physician removes the speculum with the
other gloved hand and proceeds to conduct a postoperative bimanual
examination. If the uterine size seems larger than expected, the
physician should replace the speculum and determine whether, in fact,
the procedure has not been completed… As I complete the bimanual
examination, I ask each patient to place the fingertips of both her
hands over the uterus and rub constantly for 2 hours… this will
help the uterus to contract and thereby stop the bleeding and
cramps.6
After
the examination is finished, Hern reassures the woman that "she is no longer
pregnant." According to Hern, many of them cry.7
EARLY
MEDICAL ABORTION:
The Stats:
 Medical abortion describes another method of abortion usually used in the first months of pregnancy. The drug used is Mifepristone,
sometimes also called RU486, which prohibits the hormone progesterone from functioning properly. 6
Medical abortion describes another method of abortion usually used in the first months of pregnancy. The drug used is Mifepristone,
sometimes also called RU486, which prohibits the hormone progesterone from functioning properly. 6
Medical
abortion is often advertised as a more-natural procedure than surgical abortion. Although the National Abortion Federation (NAF)
emphasizes that there is no moral difference between
medical abortion and surgical abortion. They write:
Some
patients report that they prefer the medical abortion because it
seems like a heavy period or a miscarriage rather than an abortion…
It is important for the patient's postabortion
well-being that
she does not fool herself (into thinking she is not having an
abortion) and that the provider does not participate in her
self-deception.8
According
to the NAF statistics, women who choose medical abortion "like that it is
noninvasive and offers more privacy and control," while those
who choose surgical abortion do so "because it is quick,
predictable, and may be combined with sedation or anesthesia."9
The Procedure:
 This drug takes a three week process to complete abortion. If it fails a surgical abortion is then scheduled, which the patient signs for before medical abortion is performed.
This drug takes a three week process to complete abortion. If it fails a surgical abortion is then scheduled, which the patient signs for before medical abortion is performed.
Unlike surgical abortion, women who medically abort most often see the embryo upon abortion. Physicians are told to explain this fact to their patients, since patients likely will recognize a body. These women are shown true to life size illustrations of the embryos (or "products of conception as the NAF states) to avoid potential trauma. 10
Embryo: Unborn child after the third week of conception.
Fetus: A term given to the embryo after week 8.
NAF: National Abortion Federation. North America's official providers for abortion.
1st Trimester: Week 0-12
2nd Trimester: Week 13-27
3rd Trimester: Week 28- end of pregnancy (about 42 weeks)
Gestation: The process of carrying or being carried in the womb between conception and birth.
Planned Parenthood: In 1921 feminist Margaret Sanger first founded the American Birth Control League which later became Planned Parenthood Federation of America in 1941. Planned Parenthood has since grown to have over 820 abortion clinics in the US with a total budget of $1 billion.
Abortion: ...to be decided
~ * ~
DILATION
AND EVACUATION (D&E) ABORTION:
The Stats:
Worldwide 15% of all abortions are performed after the 2nd trimester.11 That's a little over 150,000 a year, in the United States alone. It is amazing to note that 96% of all second trimester abortions are performed by the D&E method.12
The
National Abortion Federation (NAF) reports that most women seeking
second-trimester abortion are young and healthy.13 Serious
health problems account for only a small proportion of abortions
worldwide.14 According
to the NAF, the most common reasons for a second-trimester abortion given are, denial or delay in recognizing pregnancy, financial difficulty for obtaining abortion, indecision, or
changed circumstances.15
The Procedure:
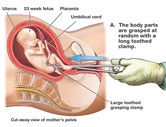
To describe the procedure of D&E abortion: Forceps are inserted through the dilated cervix for the dismemberment and removal of the human fetus. This requires a 10-12 mm cervical dilation. But for gestations 17 weeks or more longer and heavier forceps must be used.
The NAF reports that "Bierer forceps are the
weightiest and largest-jawed [with] fenestrated and sharply serrated
jaws (to) provide the most traction."16 The
NAF recommends that ultrasound guidance be used "in cases that
require a considerable degree of force to remove fetal parts."17 This
helps ensure that the abortionist does not accidentally grasp and
tear the myometrium (uterine
wall) while grasping and tearing apart the fetus.
 The
National Abortion Federation instructions for a D&E abortion are
as follows:
The
National Abortion Federation instructions for a D&E abortion are
as follows:
Once
the forceps has passed through the internal
os,
open the jaws as widely as possible to encircle the fetal tissue and
avoid pushing fetal parts deeper into the fundus…
After 16 weeks' gestation, fetal skeletal development is such that
the surgeon can manually sense the presence of fetal parts within the
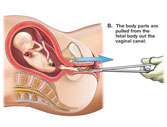
closed jaws… After grasping a fetal part, withdraw the forceps
while gently rotating it. This maneuver brings the fetus into the
lower uterine segment before the grasped fetal part is separated (if
necessary) and removed from the cervix… If a fetal extremity is
brought through the cervix without separation, advance the forceps
beyond the extremity to grasp part of the fetal trunk. Bringing the
fetal trunk into the lower segment markedly reduces the number of
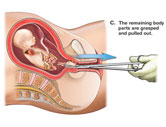
instrument passes into the fundus… During the procedure, try to
identify and keep track of fetal parts as they are removed. A "pouch'
or surgical pan at the edge of the gable to catch fetal parts can
assist this process."18
The Doctor's Description:
Warren
Hern, who the NAF credits as being an "American innovator"65 in
D&E technique, offers the following instruction:
It
is better to use smaller forceps and take smaller amounts of tissue
each time than to deliver fetal parts intact while traumatizing the
cervix… At 16 to 17 weeks, fetal tissue is much more easily
identifiable with the forceps and in some ways is easier to grasp and
remove than in earlier gestations. The [skull] is about the size of a
Ping-Pong ball and usually can be grasped readily with the Bierer.
Collapsing it gives a definite sensation… At 18-19 menstrual weeks…
fetal parts are significantly larger and more difficult
to morcellate(tear
into pieces)… [Abortion after the] 20-week gestation… can be a
significantly more difficult procedure accompanied by unnerving
hemorrhage. Forceps use must be sure and relatively rapid. There is
frequently not much time for exploring the nuances of different
tissue sensations. Grasping and collapsing the [skull is] often
difficult. Stripping the [skull] of soft tissue is sometimes the
first step in successful delivery of this part, followed by
dislocation of parietal bones. In this case, care must be taken in
removal because ossification is occurring and the edges are sharp…
Regardless of the amount of dilatation, delivery of the [skull] and
pelvis is sometimes difficult… The advantage obtained by having a
softened cervix could become a disaster if a laceration develops at
the level of the internal os as the result of too much force… The
procedure changes significantly at 21 weeks because the fetal tissues
become much more cohesive and difficult to dismember. This problem is
accentuated by the fact that the fetal pelvis may be as much as 5 cm
in width… [The skull] can be collapsed. Other structures, such as
the pelvis, present more difficulty… A long curved Mayo scissors
may be necessary to decapitate and dismember the fetus, since it may
be impossible to apply forceps or to do so while avoiding the
thinned-out cervix."19
To verify a complete abortion the fetal parts must be examined. The foot is often measured to "estimate
gestational age after abortion."20
Foot photo at 13 weeks
DILATION
AND EXTRACTION (D&X) OR PARTIAL BIRTH ABORTION:
The Stats:
Dilation
and Extraction (D&X) is a variant of D&E. In contrast of the D&E's piece by piece method, D&X delivers the aborted fetus intact and therefore is sometimes called "intact D&E" as in The Partial Birth Abortion Ban Act of 2003 . Politically, it is known as partial-birth abortion.
The Procedure:
The syllabus of the Partial Birth Abortion Ban Act describes the difference between "usual" D&E technique and "intact D&E" this way:
In the usual second-trimester procedure, “dilation and evacuation” (D&E), the doctor dilates the cervix and then inserts surgical instruments into the uterus and maneuvers them to grab the fetus and pull it back through the cervix and vagina. The fetus is usually ripped apart as it is removed, and the doctor may take 10 to 15 passes to remove it in its entirety. The procedure that prompted the federal Act and various state statutes, including Nebraska’s, is a variation of the standard D&E, and is herein referred to as “intact D&E.” The main difference between the two procedures is that in intact D&E a doctor extracts the fetus intact or largely intact with only a few passes, pulling out its entire body instead of ripping it apart. In order to allow the head to pass through the cervix, the doctor typically pierces or crushes the skull.21
The
National Abortion Federation (NAF) describes D&X:
Because
the cranium represents the largest and least compressible structure,
it often requires decompression… Decompression can be accomplished
with forceps or by making an incision at he base of the skull through
which the intracranial contents are suctioned. If the fetus is in
cephalic presentation (head first) with the calvarium well-applied to
the cervix, the surgeon can pierce the calvarium with a sharp
instrument and collapse it externally.22
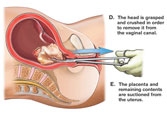
If the fetus is delivered feet first the baby's head is crushed with forceps or pierced with scissors. The brain is then suctioned out by a vacuum aspirator.
If the baby is delivered head first the head is pierced with scissors as soon as the head appears.
The Doctor's Description:
Warren Hern, who developed the Hern
forceps, writes this in Abortion
Practice:
Cervical
obstruction by the calvaria (skull) is a paradoxical problem, since
it is the opposite of having difficulty in recovering tissue… Small
instruments cannot encompass it; large instruments… either push it
away, cannot be closed once the [skull] is grasped, or, having
grasped the [skull], cannot be withdrawn. Unless the [skull] can be
collapsed and delivered, however, the procedure cannot be completed…
and the risk of complications begin to increase. The most useful
maneuver in this case is to grasp the presenting of the [skull] with
the cervical tenaculum, stripping away the soft tissue (skin). When
the skull bones are visible, they are grasped also with the
tenaculum. A long curved Mayo scissors is then used to dissect the
[skull] to the point that it is opened and decompressed. At this
time, a forceps with a very strong blade and firm grasp… may be
used to grasp the tentorium and skull plates, sometimes dismembering
by torsion and sometimes by sharp dissection with the Mayo
(scissors)… Once some dismemberment has taken place, the operator
may take a somewhat larger forceps… As the tissue is pushed
slightly up in to the uterine cavity, the forceps blade is opened and
a moderate amount of tissue is grasped… With good dilatation and
effacement, the entire fetus may be delivered.23
In 2007 the Supreme Court upheld the Partial Birth Abortion Ban Act of 2003, which states: "punctur[ing] the back of [a] child's skull with a Sharp
instrument, and suck[ing] the child's brains out before completing
delivery of the dead infant -- is a gruesome and inhumane procedure
that is never medically necessary and should be prohibited."24
The NAF
condemns both Congress and the Supreme Court for "denying
reproductive freedom"25 and "ignor[ing] the best
judgment of the medical community."26 Included among their
reasons for why D&X can be more advantageous than D&E is the
assertion that it "permit(s) more complete morphologic
evaluation of an extracted fetus,"27 it "minimizes the
risk of retained tissue,"28 and it gives grieving parents
"the opportunity to view or hold an intact fetus."29
While D&X is prohibited, the Partial Birth Abortion Ban can be circumvented.
The NAF advises
abortionists to kill the baby by injection prior to performing a D&X
procedure. According to the language of the Ban, it is "applicable
only when a 'living fetus' is present at the outset of
evacuation."30
The NAF offers the following advice for
killing babies by injection:
Digoxin
in doses of 1.0 to 1.5 mg appears to effect fetal demise. Providers
may feel a change in resistance at the needle tip as it enters the
fetus. Unless the needle is in the fetal cardiac chambers, aspiration
will not usually yield fetal blood… fetal demise occurred in 43% at
2 hours; 75% at 3 hours , and 98% in 5 hours… Potassium chloride
will not achieve fetal demise when injected into the amniotic fluid;
injection into the fetal heart or umbilical cord is required…
Needle placement should be maintained until fetal death is confirmed
monographically. These technically challenging procedures are
performed most commonly for multifetal pregnancy reduction…
Clinicians typically administer agents to cause fetal demise 1 to 2
days before D&E, often in conjunction with cervical
preparation.31
So, what is abortion? It's
destruction...legal premeditated murder. A heinous crime. Termination; a cruel tortuous death performed upon an innocent.
Now you know.
So what are you going to do about it?









