Political/World Issues
Health and Beauty
Ectopic/tubal
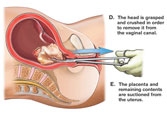
Pregnancy Abortion
Recently, I was addressed with the question: "Is abortion acceptable in a case of Ectopic/tubal pregnancy?" Honestly, I didn't know that much about it. All I could really say on the subject was what I’d just heard from other people’s perception of it. So, today I did my research. I was amazed by what I learned. The truth is, the more I study and educate myself about health in general, the more I see why it is so important to do so. You almost have to be your own doctor, because you cannot simply believe what others will tell you or blindly follow the flow of society. I hope this information is maybe helpful to you, and if nothing else, educational. So, I would encourage you, reader, to research and to study for yourself. It is good to know what we believe and why.
So, what is Ectopic Pregnancy?
Definition of
ectopic
- Pregnancy with the fertilized embryo implanted on any tissue other than the uterine lining
- 95% of ectopics are in the tube, 1.5% abdominal, 0.5% ovarian and 0.03% are in the cervix
- Only a 2% chance that a pregnancy will be Ectopic/tubal
My perception
of "Ectopic/tubal pregnancy" from all I'd ever heard was that it was
a case where, if not somehow prevented, the baby would inevitably always die
and the mother could possibly then die as well. MOST people think this is true
and therefore use an abortive, either drug or surgery, to immediately end the
pregnancy. If the baby is dying anyway, and the life of the mother is therefore
then put at risk, why would you hesitate to abort the baby? Although this
thinking logically does make sense, it didn't sit right with me. How could it ever
be acceptable to murder a baby? It couldn't be.
Every
"medical website" said the same thing. With Ectopic pregnancy there
is no other option than to abort the baby immediately before you put yourself
at fatal risk. The doctors would advocate that you go in for
emergency abortive surgery. A few websites admitted to certain
"exceptions" or "rare cases" where the baby somehow
survived outside the mother's uterus. But those were rare and somewhat
unacceptable.
When I came
across a story of a mother that safely kept her Ectopic baby full term, I was
pleasantly surprised and it opened an avenue of information! Here is
the account:
Rare
baby survives outside womb: Montreal doctor
CBC
News Posted: Aug 12, 2003 10:16 AM ET Last Updated: Aug 12, 2003
10:16 AM ET
 Surgeons in Montreal performed a C-section
and found a baby managed to grow and develop outside his mother's uterus. Dionne
Grant, 29, and her newborn son should be going home later this week. Although
she is camera shy, Grant wanted the world to see her baby. He does not yet have
a name. Dr. Robert Sabbah, head of obstetrics and gynecology at Sacr-Coeur
Hospital, said he only discovered the problem after deciding to perform an
emergency caesarean section on the Jamaican tourist last week.
Surgeons in Montreal performed a C-section
and found a baby managed to grow and develop outside his mother's uterus. Dionne
Grant, 29, and her newborn son should be going home later this week. Although
she is camera shy, Grant wanted the world to see her baby. He does not yet have
a name. Dr. Robert Sabbah, head of obstetrics and gynecology at Sacr-Coeur
Hospital, said he only discovered the problem after deciding to perform an
emergency caesarean section on the Jamaican tourist last week.
"When I opened the cavity I quickly
discovered that the uterus was not like it was supposed to be," said
Sabbah. "As soon as I explored the abdominal cavity I noticed there were
feet in the cavity just floating around. So as fast as I could I took out the
baby."
He said that abdominal ectopic pregnancies
occur in one in 10,000 pregnancies. In 99 per cent of the cases, the babies
die. There are only a dozen similar cases in the world, according to
obstetricians. Doctors believe the baby survived because the placenta glued
itself to the top of the uterus, accessing blood to nourish the baby. Sabbah
said he's thrilled to have been part of the surgery and even more thrilled that
both his patients are doing so well.

A more accurate percentage could be obtained by considering that deaths associated with ectopic pregnancies only make up about 6% of the yearly maternal deaths in America. If this figure were to be applied to the maternal mortality rate of southern Israel, we would derive that there were .03 ectopic related deaths per year for that region. When that figure is divided by an average of 4.8 tubal ruptures per year, we arrive at the conclusion that a woman in southern Israel has a 99.4% chance of surviving an ectopic pregnancy which is not aborted prior to rupture.
A similar calculation for America produces a lowest possible minimum of 97.7% survival.
In addition, we could calculate the maternal risk from the total number of heterotopic pregnancies (twins with one child in the womb and the other being ectopic) in America. According to Dr. Tenore of the Northwestern University Medical School in Chicago, this type of pregnancy occurs in 1 out of every 2,600 pregnancies, and 50% of them (1 out of every 5,200 pregnancies) "are identified only after tubal rupture." According to the American Pregnancy Association, there are approximately 6 million pregnancies per year in the US. Therefore, there are an average of 1,154 heterotopic pregnancies every year in America which are not even discovered much less treated prior to tubal rupture. The CDC reported that there are an average of 26.3 maternal deaths per year that are ectopic related. If we assumed that all of these ectopic related deaths were the result of an undiagnosed heterotopic pregnancy (a condition which only makes up 1% of the total number of ectopic pregnancies), then we would still arrive at a maternal survival rate of 97.7%.
Ectopic/tubal
pregnancy baby survivors actually aren't as impossible as I would have thought.
I think the reason they are more uncommon, is because woman are told that the
"abortion of the baby" is the ONLY option and therefore, the baby is
never even given the chance to try to live. I was shocked by how many stories I
came across where the mother actually was somehow able to carry her baby even
outside the uterus lining. Weird. But it is possible. It is most common,
however, that the baby will naturally die. At approximately 8 to 9 weeks most
tubal pregnancies will rupture. This can be dangerous for the mother, with
risks of hemorrhaging, internal bleeding, and possible infection, and it
is extremely important that she gets medical help; although, it is still
not unheard of that both the baby and the mother survives even a tubal rupture.
(I'm honestly unsure how that works, but I do believe the baby has to be past
28 weeks.)
So,
is it actually as dangerous a threat to the mother's life as is commonly made
out to be?
No, not
really. And while there is a chance that the mother could die, it isn't as high
as I would have thought. I found this particular website, and the
information from it, extremely helpful. http://www.personhoodinitiative.com/articles.html
The actual survival rate is more likely to
be 99.4%.
A more accurate percentage could be obtained by considering that deaths associated with ectopic pregnancies only make up about 6% of the yearly maternal deaths in America. If this figure were to be applied to the maternal mortality rate of southern Israel, we would derive that there were .03 ectopic related deaths per year for that region. When that figure is divided by an average of 4.8 tubal ruptures per year, we arrive at the conclusion that a woman in southern Israel has a 99.4% chance of surviving an ectopic pregnancy which is not aborted prior to rupture.
A similar calculation for America produces a lowest possible minimum of 97.7% survival.
In addition, we could calculate the maternal risk from the total number of heterotopic pregnancies (twins with one child in the womb and the other being ectopic) in America. According to Dr. Tenore of the Northwestern University Medical School in Chicago, this type of pregnancy occurs in 1 out of every 2,600 pregnancies, and 50% of them (1 out of every 5,200 pregnancies) "are identified only after tubal rupture." According to the American Pregnancy Association, there are approximately 6 million pregnancies per year in the US. Therefore, there are an average of 1,154 heterotopic pregnancies every year in America which are not even discovered much less treated prior to tubal rupture. The CDC reported that there are an average of 26.3 maternal deaths per year that are ectopic related. If we assumed that all of these ectopic related deaths were the result of an undiagnosed heterotopic pregnancy (a condition which only makes up 1% of the total number of ectopic pregnancies), then we would still arrive at a maternal survival rate of 97.7%.
The claim that an unborn child cannot survive an Ectopic pregnancy:
 a. Between 1809 and 1935, there were 316 reported live births from ectopic
pregnancies.
a. Between 1809 and 1935, there were 316 reported live births from ectopic
pregnancies.
Two OBGYNs in New York, Dr.’s Hellman and Simon,
published details on 316 ectopic pregnancies which resulted in live births
between 1809 and 1935. Only half of these children survived their first
week of life, but these births occurred before the development of the first
neonatal intensive care unit, and most of them before the discovery of
penicillin in 1928. With modern technology, it is likely that many more
would have survived.
b. With modern technology, there have been even more of these births in recent years in spite of the insistence that abortion is the only viable treatment.
b. With modern technology, there have been even more of these births in recent years in spite of the insistence that abortion is the only viable treatment.
In September of 1999, Ronan Ingram was successfully delivered via c-section. Ronan had implanted in one of his mother’s fallopian tubes which subsequently ruptured as he grew into the abdominal cavity. In May of 2008, Durga Thangarajah was born after spending a full nine months in her mother’s ovary. Sage Dalton was born in July of 1999 after developing in the amniotic membrane outside her mother’s womb. Billy Jones was born in 2008 after developing in his mother’s abdominal cavity. Many additional reports could be given.
The
claim that termination is the only treatment for ectopic pregnancies that is
recognized by the medical profession:
Many OBGYNs have recommended allowing ectopic pregnancies to resolve on their own.
Dr.’s Sapuri and Klufio, for example, have recommended that women discovered to have an ectopic pregnancy prior to 28 weeks of gestation should be admitted to a hospital and closely monitored. They stress that blood transfusion facilities should be readily available in case of hemorrhage, and they suggest that once the child has reached 28 weeks of gestation, he should be delivered surgically.
Many OBGYNs have recommended allowing ectopic pregnancies to resolve on their own.
Dr.’s Sapuri and Klufio, for example, have recommended that women discovered to have an ectopic pregnancy prior to 28 weeks of gestation should be admitted to a hospital and closely monitored. They stress that blood transfusion facilities should be readily available in case of hemorrhage, and they suggest that once the child has reached 28 weeks of gestation, he should be delivered surgically.
An
Ectopic/tubal pregnancy certainly could be dangerous and definitely isn't
ideal, but it isn't impossible either. Abortion isn't the only option, as
doctors conclude and people ignorantly and blindly believe. It shouldn't even be an
option. If there is still a possibility that you could save your Ectopic/tubal pregnancy...why
wouldn't you try? If there was even a small chance that you could somehow keep the life of your baby, isn't that something to consider? To most doctors and pro-choice representatives, it is seen only as a "blob of tissue" that
could possibly be a fatal risk, so they insist on immediate removal. And I think maybe even most pro-life christians just blindly believe what the doctor tells them to do. But it is a life. And outside the mother's uterus or not, it is worth fighting for.